Sahar A Fahmy1 ![]() ,
Eman Abu-Gharbieh2,
Samer Hamidi3
,
Eman Abu-Gharbieh2,
Samer Hamidi3
For correspondence:- Sahar Fahmy Email: sahar33a@hotmail.com
Received: 7 October 2015 Accepted: 30 March 2016 Published: 27 May 2016
Citation: Fahmy SA, Abu-Gharbieh E, Hamidi S. Patterns of prescribing and utilization of asthma medications in a tertiary hospital in Dubai, United Arab Emirates. Trop J Pharm Res 2016; 15(5):1061-1068 doi: 10.4314/tjpr.v15i5.23
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To assess the prescribing patterns of asthma medications in a hospital in Dubai, United Arab Emirates (UAE) with regard to the demographic pattern of the population.
Methods: One hundred fifty four patients, 83 male and 71 female, were randomly selected from the outpatient respiratory diseases clinic of a tertiary hospital in Dubai, UAE over a 3-month period. Patients were asked to complete a structured questionnaire and data were analyzed using STATA 12 software.
Results: Most of the patients were within the age range of 0 – 10 years. About 86 % of the patients were overweight. Half of the patients were non-smokers while 51 % of them had a family history of asthma. About 54 % of the patients received multiple drug therapy of which two-drug combinations were widely prescribed (31 %). The most utilized drug classes were short acting β-agonists (42 %), xanthine drugs (16 %), leukotriene modifiers (14 %) and oral and intravenous corticosteroids (13 %). Statistical significant differences among the age groups (F = 2.33, p = 0.0275) were found.
Conclusion: Primary prevention to reduce the level of exposure to common risk factors for asthma would be a vital step to control the disease. More resources should be channeled into educating physicians and patients on rational drug utilization to improve the quality of patients’ care.
Introduction
Drugs play an important role in improving human health and promoting well-being if used rationally. Drug utilization reviews (DUR) provide a powerful tool to assess knowledge and awareness of patients and physicians on the proper use of medications [1]. DUR is increasingly used as a tool for cost containment and quality assurance. There are three types of DUR reviews which are prospective, concurrent and retrospective. DURs help regulators implement the appropriate interventions to address certain issues in the health care systems. Among which is designing educational programs to improve prescribing practice and developing standard treatment protocols to treat specific diseases [2].
Asthma is a condition in which recurrent attacks of breathlessness and wheezing occurred mainly due to inflammation of the air passages. During asthma attack, airways are narrowed due to swelling of the lining of the passages causing reduction of the air flow [3]. In 2013 World Health Organization (WHO) estimated that 235 million people (3.5 percent of the world's population) currently suffer from asthma, and it is considered as the most common non-communicable disease among children [3]. The report on the global burden of asthma estimated that the number of disability-adjusted life years (DALYs) lost due to asthma was estimated to be around 15 million DALYs per year, and accounted for around one in every 250 deaths worldwide [4]. In UAE, asthma is considered one of the most predominant disease with about 8 % to 10 % of adults are suffering from asthma [5]. It was also reported that about 53 % of children, and 17 % of adults were missing school and work, respectively, due to asthma [6].
In another study conducted in Abu Dhabi, the capital of UAE, it was reported that around 10 % of patients had made an emergency room visit because of Asthma. The direct cost of treating asthma in Abu Dhabi was estimated to be about 105 million AED a year, with 31 % cost spent on medications only [7].
In the current study we investigated the pattern of drug use for asthma medications taking into consideration the demographic variations among patient population. This is done by conducting prescription audits and identifies irrationality in drug prescribing. Our main aim is to set recommendations for health regulators in order to take the appropriate measures to improve prescribing and hence improve quality of patient care.
Methods
An observational study was planned to analyze the utilization patterns of anti-asthmatic drugs in a tertiary hospital in Dubai, UAE. The protocol of the study protocol was approved by hospital administration to conduct the study in the hospital. Two hundred patients visiting the out-patient respiratory diseases clinics were randomly selected during a period of three months (September to December 2012). Patients seen in the specialized clinics are followed up by respiratory diseases specialists or consultants. Data were collected through a structured questionnaire targeted asthmatic patients. The questionnaire was composed of two sections; the first set of questions were concerning patient demographic data i.e. age sex, occupation, level of education, family history and smoking status. The second set of questions captured all relevant information related to the prescribed medications with dosing, frequency and route of administration.
Inclusion criteria
Patients diagnosed with asthma and are currently on anti-asthmatic medications were included in the study.
Exclusion criteria
Asthmatic patients who suffered from other diseases such as hypertension, diabetes, heart problems, bronchitis, chronic obstructive pulmonary disease (COPD), peptic ulcer, diabetes mellitus or any other co-morbidities were excluded.
Patients were randomly recruited in the study and they signed the informed consent form to indicate their participation in the study. They were interviewed and necessary information was collected as per the structured questionnaire. The prescriptions of participated patients diagnosed with asthma were collected and were interviewed for different parameters.
Statistical analysis
Descriptive statistics were carried out for all assessed parameters and results were expressed as frequencies and percentages. The data were analyzed for different parameters using One-way analysis of variance (ANOVA). P < 0.05 was taken to denote statistical significance. All statistical analysis was conducted using STATA (StataCorp, College Station, Texas, US) version 12.
Results
Demographic characteristics
Among the 200 randomly selected patients, only 154 patients were eligible to be included in the study as per the inclusion criteria. Around 54 % of the study population was males with most of the patients diagnosed with asthma were within the young age group (0-10) years. About 86 % of the patients were overweight. Most of the patients are well educated with 54.6 % of patients have graduate degree. About 23 % of patients were UAE nationals and about 77 % were expatriates. Patient smoking history was assessed and determined to be of equal distribution among patients with 51 % of patients were none smokers. About 51.3 % of patients had a family history of asthma. The majority of patients participated in the study (76.6 %) were with upper middle socioeconomic status. summarizes patients’ demographic data.
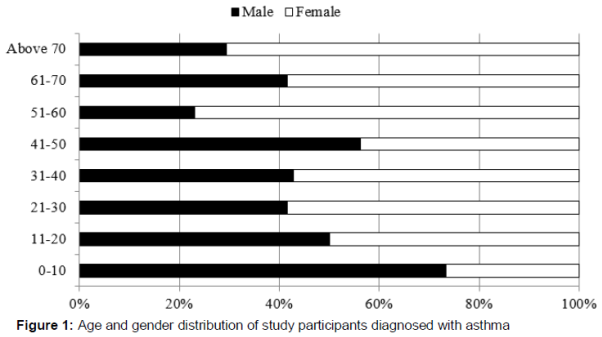
Age-gender distribution of patients diagnosed with asthma
To capture the age gender distribution among participants, gender data was analyzed for the eight age groups. It was found that male group were highly distributed within two age groups with 46 (72 %) and 9 (56 %) study participants aged between (0-10) years and (40-50) years respectively. However, the female group was highly distributed within two age group with 10 (77 %) and 12 (71 %) of study participants aged between (51-60) years and (above 70) years respectively. , shows age and gender distribution of patients with asthma. A statistical analysis was done for age- gender distribution using (ANOVA) and the results showed a significant difference of gender distribution among the different age groups with a p- value of 0.0275.
A total of 83 (54 %) of study participants received multiple drug therapy compared to 71 (46 %) of participants who received single drug therapy. In multiple drug therapy, two-drug combinations were widely prescribed 48 (31 %) than combinations of three 24 (16 %) or four drugs 11 (7 %) as shown in .
The pattern of drug prescription for treating asthma at the study showed that short acting β-agonist (SABA) are the highest prescribed class of medications (42 %) followed by xanthines (16 %),leukotriene modifiers (14 %) and corticosteroids (13 %) as shown in .
The most commonly prescribed drug was Combivent® which is composed of salbutamol and ipratropium bromide with a ratio of 23 % followed by Ventolin® (salbutamol, 16 %) and Singular® (montelukast, 14 %) as shown in . Salbutamol or albuterol were chosen as the first line drug in the management of asthma and were used as required by patients for the symptomatic relief of breathlessness and wheezing.
The use of all asthma medication classes was determined to be significantly different among the different age group (F = 2.33, p = 0.0275). The 0 – 10 years age group showed the highest rate of drug utilization (32 %).
Drug utilization was assessed based on gender distribution and found to around (47 %) for males versus (53 %) for females. There was no statistical significant difference among male and female patients in terms of utilizations of asthma medications (F = 2.55, p = 0.1124).
Discussion
Drug therapy is used to relieve and prevent symptoms of asthma and treat exacerbations. Results of the study showed that drug classes commonly used to treat asthma include short-acting beta agonists which are used for short-term symptom relief; xanthine drugs, leukotriene modifiers, oral and intravenous corticosteroids which are used during episodes of more severe asthma; and inhaled corticosteroids and long-acting beta agonists, used for symptom prevention and disease control. Over the years, inhaled corticosteroids have dominated asthma treatment [8]. However, medical reports showed that the more the asthma patients used inhaled steroids, the weaker their bones became, thus increasing the risk of osteoporosis [9].
Most people who are on inhaled corticosteroids use them intermittently, even though guidelines recommend that these drugs be used regularly by those who need them [10]. Most adults also use the strongest formulations of inhaled corticosteroids, even though less potent formulations are often effective and have fewer side effects [10]. The results showed that about only 9 % of patients use inhaled corticosteroids, which is a good sign of rational drug utilization.
Another therapeutic category used for the management of asthma is leukotriene modifiers with 14 % of study participants on the treatment alone or in combination with other medications. The ability of leukotriene receptor antagonist-based medication, to be used along with inhaled beta-agonists or added to existing asthma treatment regimens; allow reduction of a concomitant therapy. Innovative drugs are the leukotriene receptor antagonists which are playing an important role in asthma therapy and offer advantages over other currently available treatments, including excellent tolerability, oral route of administration, once-daily dosage and proven efficacy in a wide range of patients, including children.
The use of short acting drug relievers alone was evidenced not to control asthma properly. People with asthma who rely on short-acting beta agonists, without using inhaled corticosteroids, have been shown to be more likely to suffer exacerbations or attacks of asthma requiring an emergency department visit or an admission to hospital [11]. In our study most of study participants received salbutamol. Salbutamol is the preferred Short acting beta-2 agonist because it has an excellent safety profile. Rapid reversal of airflow obstruction is best achieved by repetitive administration of salbutamol nebulisation which is considered to be the first medication of choice and it is lifesaving.
Utilization of asthma medication was highest in early childhood from the age range of (0-10 years) and late in elderly (over 70 years). This might be due the fact that elderly are especially prone to the adverse health effects of chronic obstructive pulmonary disease (COPD), which is a common disorder in that population [12].
Limitations of the study
The study was conducted in one hospital only. Expanding the study to different settings is needed to assess prescribing practices in those settings. Assessment of illness severity was not possible due to lack of access to patient medical records. Thus, patients could not be classified into different groups based on severity and could not evaluate whether the prescribing patterns were in line with international standards. In addition, the effect of data based on only one visit to a patient in outpatient settings on the assessment of how prescribing patterns changed over the course of illness in patients remains unclear.
Conclusion
Asthma creates substantial burden to individuals and families and often restricts individuals’ activities for a lifetime.
The present prescribing practice in the management of asthma in the setting of this study is not sufficiently rational. The presented data should be considered a baseline for the current practice and may be used in proposing appropriate interventions to improve current prescribing trend for a more rational utilization of asthma medications. It is also recommended that to develop asthma treatment guidelines and monitor physician adherence to such guidelines in order to manage asthmatic patients effectively. More steps are required to implement regulatory and managerial interventions needed to promote rational prescribing of asthma medications.
Declarations
Acknowledgement
References
Archives


News Updates